


Breast augmentation is an operation aimed at increasing the volume of the breasts. In breast augmentation, similar to any other intervention in cosmetic surgery, careful pre-operative planning is essential, which must take into account the patient’s wishes in terms of shape and volume and evaluate whether these are feasible based on the starting anatomical situation.
We can perform the surgery with surgical access that can be from the inframammary sulcus, from the areola, or from the axillary cavity, creating a pocket that can be retroglandular, retrofascial, or retromuscular, using round or anatomical prostheses with various degrees of projection and cohesion, coated with silicone or polyurethane.
All these variables are chosen taking into account both the preoperative anatomical situation of the breasts and the patient’s wishes and must be carefully evaluated during the preliminary interviews.

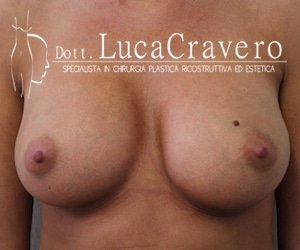
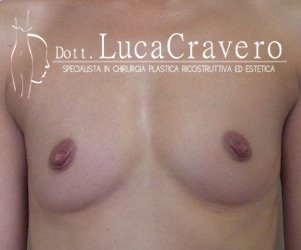
1. BEFORE AND AFTER PHOTOS (retromuscular anatomical prosthesis)
2. BEFORE AND AFTER PHOTOS (round prostheses)
3. VIDEO CASES COMMENTARY
ACCESS ROUTES
Inframammary sulcus: It is the most anatomical, most natural access: it passes under the mammary gland, under the fascia of the pectoral muscle, or under the pectoral muscle itself and not through them. It must be taken into account that at the end of the operation, the mammary sulcus has moved downwards. For this reason, there are now several algorithms which, by calculating the initial volumes, the desired volumes, and the characteristics of the skin and tissues, allow to place the incision in the new furrow to within half a centimeter maximum.
Axillary cavity: Access from the axillary cavity is the most hidden, however, due to the considerable number of hair bulbs present, the scar may be of lesser quality and therefore visible, especially in summer when wearing sleeveless clothing. Axillary access is also associated with a greater risk of malpositioning of the anatomical prostheses.
Hemiperiareolar: It is the access that, if correctly performed, tends to heal better, also because there are measures that can be adopted starting from the third month, which lead to a natural pigmentation of the periareolar scar which therefore takes on the color of the areola itself.
ACCOMMODATION PLANES
Retroglandular: It is the most natural, most anatomical plane: theoretically, if possible, all the implants should be placed directly behind the mammary gland, because it is the breast that we want to increase in volume and projection, not the muscle!
Unfortunately, in reality, patients who want breast enlargement often have very little glandular and subcutaneous coverage and therefore the retroglandular positioning would result in a substantially retrocutaneous positioning, with the risk of seeing the edge and the shape of the upper portion of the prosthesis, even taking into account a possible reduction in breast tissue volume over the years due to the compression exerted by the prosthesis itself.
Furthermore, personally, I prefer to resort to this plane very rarely and only with small and not heavy implants because there is a high risk that over time the prosthesis tends to displace downwards since the periprosthetic capsule does not have the possibility of forming tenacious adhesions.
The advantages of the retroglandular housing are:
- the speed of execution (45 minutes)
- the absence of pain
- outpatient management of the intervention
The disadvantages are:
- the greater risk of visibility of the implant
- the risk of displacement
- the increased risk of capsular contracture
Retrofascial: The prosthesis is placed between the pectoral muscle fascia and the pectoral muscle itself. It is a plane generally not used by surgeons (perhaps because it is surgically a little longer and more delicate than the retromammary housing), but if the thickness of the tissues allows it, it is an excellent method because it allows you to have the benefits of a retromuscular positioning, all thanks to the compression exerted above by the fascia of the pectoral muscle (a thin, but inextensible and very strong structure) and a retroglandular positioning (because the pectoral muscle is left in place).
The advantages are:
- the possibility of covering the upper pole of the prosthesis because the band, even if thin, is robust and inextensible and therefore makes the upper pole of the prosthesis less visible
- the stability of the result over time because the periprosthetic capsule is firm between fascia and muscle and does not tend to precipitate downwards over the years unlike in retroglandular positioning
- The absence of pain (the muscle is left in place)
The disadvantages are:
- Surgery a little longer and more delicate (often the band is thin)
- However, in the absence of adequate thickness of the subcutaneous and glandular tissues, it does not guarantee adequate coverage of the upper pole if round or even anatomical high-projection prostheses are used.
- Basically, in our opinion, the retrofascial positioning should be carried out when there are anatomical indications for a retroglandular access in order to give greater guarantees of a long-term stable result compared to a retroglandular prosthetic housing.
Retromuscular: It is the most frequently used plane because it always guarantees adequate coverage of the upper pole and gives the greatest guarantee of stability over time. The prosthesis is placed between the muscle and the rib. The plane can be totally retromuscular or partially (dual-plane).
With the first technique, the prosthesis is inserted completely behind the pectoralis major muscle and part of the dentate muscle. It is a technique particularly suitable for patients with very low breast tissue thickness, but which we tend to use little because the breast is rather hard to the touch, with a poor convexity of the lower pole and changes shape a lot with each muscle contraction.
With the second technique (Dual Plane), which we prefer when inserting the retromuscular prosthesis, we create a housing pocket for the prosthesis only behind the pectoralis major muscle without touching the other muscles of the chest wall after detaching the mammary gland from the pectoral muscle itself in a quantity proportional to how much we want to lift the gland.
With this technique, 50-75% of the prosthesis is covered by the muscle while the lower part remains in the retroglandular position.
The advantages are:
- Coverage and compression of the upper pole exerted by the pectoral muscle with the possibility of using round or anatomical prostheses with high projection without the risk of an excessive “push-up effect”
- Massage of the prosthesis by the pectoral muscle itself with reduction of the risk of capsular contracture
- Stability of the result (the capsule firmly adheres between the side and the muscle)
The disadvantages are:
- Possible deformity of the breasts when contracting the pectoral muscle
- Increased risk of high dislocation or post-surgery asymmetry (due to residual activity of the pectoral muscle that mobilizes the prostheses)
- The greater risk of having post-operative discomfort: I have deliberately written “discomfort” and not pain because, in today’s times, there is a new possibility for the intervention to avoid being painful in over 90% of cases through appropriate surgical and anesthetic measures. The risk that a normal post-operative discomfort turns into pain is certainly higher when very large volume prostheses are inserted because it inevitably increases the tension and stretching of the tissues involved.
- Greater caution in the post-operative period with regards to the gestures in which the pectoral muscles are used, which must be stressed as much as possible to avoid dislocation of the prostheses within three months following the intervention (time in which the formation of the prosthetic capsule is completed) unless polyurethane prostheses are used.
SHAPE OF THE PROSTHESES
Prostheses can have two forms:
Round shape: Actually the correct diction would be “hemispherical” because it is not round like a ball!
For us, it remains the first choice when we are faced with a well-shaped breast, with a nipple well centered on the mammary gland and when the patient likes a certain convexity of the upper pole (“push up effect”).
It is essential to emphasize that even with round prostheses, contrary to popular belief, it is possible to obtain a natural result, it depends on the starting tissues, the housing surface, and above all, on the degree of prosthetic projection (if you want a natural result it is preferable to opt for a moderate screening)
Anatomical shape (“drop”): It is the most natural shape because it follows the shape of the breast.
The choice between a round or anatomical shaped prosthesis can in some cases be left to the patient’s personal taste, but in our opinion, opting for a “teardrop” shape becomes inevitable when you want to achieve a certain lift of a ptotic breast or when a stable result is sought over the years, taking into account the fact that many breasts, especially after a certain degree of tissue deterioration (post-pregnancy, post-weight loss) tend to go down and can be more easily “supported” with an anatomical prosthesis.
DEGREE OF PROJECTION OF PROSTHESES
Both round and anatomical prostheses have different degrees of projection (light, moderate, high, very high). This means that, once the dimensions (height and width) of the implants have been established, we can, by varying the projection, vary the overall volumes.
DEGREE OF COHESIVITY OF THE PROSTHETIC GEL
The gel that fills the prosthesis has a different degree of cohesiveness, that is, of softness, according to the brand of prosthesis and according to whether it is a round or anatomical prosthesis.
In general, regardless of the brand of prosthesis, the anatomical ones have a slightly more cohesive gel than the round ones because they have to keep the “teardrop” shape.
The more cohesive gel implants are undoubtedly preferable when the chest is very flat and the tissues are under tension because we must give the correct shape to the new breast that remains stable and contrasts the external tissue tension (for example in the outcomes of oncological demolition or severe hypomastia).
There are also anatomical double-chamber prostheses, with a softer gel posterior chamber so that the prosthesis naturally accompanies the movement of the side and a more cohesive gel anterior to better maintain the shape and raise the mammary gland more.
COATING OF THE PROSTHESES: SILICONE or POLYURETHANE?
Breast implants are all silicone content, while the external coating can be schematically divided into:
Textured silicone: The texturization indicates the degree of roughness of the prosthesis, the greater the texturization the higher the risk of inflammatory response that will lead to a more rapid formation of a peri-prosthetic capsule.
It is clear that, for an anatomical shape, an important texturing is required to prevent the prosthesis from rotating, while for a round shape, any rotation is not a problem, so it is possible to cover them with a light texture (even for some years, smooth round prostheses are back “in fashion”, ie without any roughness of the envelope, which had been almost abandoned in the 1980s as they were associated with a greater risk of capsular contracture and replaced by textured prostheses).
Polyurethane: Polyurethane prostheses have existed since the late 1970s and are routinely used in secondary operations when it is necessary to replace silicone-coated prostheses for complications such as dislocation, rotation, or capsular contracture. Even today, however, they are rarely proposed in the first instance, probably because they are more complex to implant and since they adhere very quickly and tenaciously to the tissues, they have no room for settling and therefore, if they are not positioned perfectly, they cannot be adjusted in the post-operative period until the polyurethane begins to melt noticeably.
Advantages of polyurethane prostheses:
- They have better adhesion to the tissues thanks to a very porous surface and this means that they cannot rotate or displace.
- They have a very low risk of capsular contracture, around 2-4% 10 years after surgery (Long-term safety and efficacy of polyurethane foam-covered breast implants, Handel N et al: Aesthet Surg J. 2006 May-Jun; 26 (3), while for silicone-coated implants of the main brands on the market (Allergan®, Mentor®, Sientra, ®), the risk is around 12-20% (Long-term safety of textured and smooth Breast implants, Calobrace, et al: Aesthetic Surgery journal 2018, Vol. 38 (1). The low index of capsular contracture is attributed to the internal growth and microencapsulation of fibroblasts in the polyurethane foam matrix. Unlike prostheses with both smooth and textured surfaces, around which a single large capsule is created, polyurethane prostheses promote the growth of numerous microcapsules around the foam, which is why the linear contractile forces that can disfigure the prosthesis are neutralized.
- They allow for faster recovery than silicone-coated implants. Therefore, if the patient wants a quick return to sports and/or work activity and/or uses her upper limbs for work, or if she is a mother with young children, we recommend polyurethane-coated prostheses that can be fixed in a few days to the surrounding tissues in an immovable way, eliminating the risk of rotation, elevation or asymmetry of the prostheses themselves.
- They are the gold standard in secondary interventions precisely because they are not subject to capsular contracture.
Disadvantages of polyurethane prostheses:
- It requires experience and precision on the part of the surgeon as in the event of an error, they are not easily removable, at least until the polyurethane has partially dissolved (at least 6 months). After one year from the implant, the polyurethane has reabsorbed and it is possible to remove the implant very easily because the prostheses have become substantially smooth.
- After the surgery, they may have a somewhat rigid appearance and even to the touch. There is a certain sensation of hardness precisely because the polyurethane adheres strongly to the neighboring tissues; within two / three months the polyurethane begins resorption and the prostheses soften.
- They may be slightly less suitable in very thin patients because the edges may be palpable.
Smooth silicone: The advent of texturization in the 80s marked an epochal turning point in terms of reducing the most well-known complication of breast augmentation surgery which was and still remains today, the periprosthetic capsular contracture. The smooth surface prostheses used up to those years were supplanted by another type of rough surface prosthesis (technically defined as textured) which, by this more micro-wavy surface, were probably able to limit the effects of periprosthetic scar contracture (the capsule is nothing more than a three-dimensional scar) and therefore also to reduce the risk of hardening of the prosthetic breast, following a severe periprosthetic capsular contracture, an event with smooth prostheses of the past.
A further step forward in the production of breast implants for breast augmentation occurred with the introduction of a new type of so-called teardrop or anatomical prosthesis due to its more flattened shape at the upper pole and more projected at the lower pole. But the main fact was the quality of the silicone with which the anatomical prostheses intended primarily for post-mastectomy breast reconstruction were exclusively structured, then routinely used also for breast augmentation for aesthetic purposes.
The smooth round prostheses, on the other hand, had remained behind and that is still structured always with silicone with a low coefficient of cohesion and therefore were particularly subject to the exudation of silicone from the prosthetic surface, the so-called bleeding which was the main cause of periprosthetic capsular contracture given the particular reactivity of the tissues with this type of particularly fluid silicone. For some years, that is, since the industry has also put on the market round prostheses structured with the same type of silicone as the anatomical prostheses, there is a tendency to return to round prostheses with a smooth or nanotextured surface, that is, with a very tenuous texture. This is because if it is true that at the beginning and the advent on the market of rough surface systems (at the beginning always round) seemed to have responded positively to the problem, then the introduction of anatomical prostheses showed that the reduction of contracture was linked to the quality of silicone (particularly cohesive) that did not exude from the prostheses and not only to the type of surface (textured instead of smooth).
Advantages of the smooth surface:
- Ease of insertion.
- Lower risk of wrinkling than textured prostheses that, by virtue of the particular adherence of the textured surface to the tissues above the prosthesis (Velcron effect), especially in lean subjects can make evident on the surface the natural undulations of the prosthetic surface forced in the physiological periprosthetic capsule.
Disadvantages of the smooth surface:
- They have been used only for some years, the scientific data concerning the main complication of smooth surface breast implants, capsular contracture, are still small and discordant.
- The shape of the smooth surface implants can be exclusively round (an anatomical shape would have the problem of rotation)
LET’S TAKE A FEW EXAMPLES
If the patient has breasts already well-represented with good coverage of fibroglandular tissue of the upper pole, it is possible to place the prostheses in the retroglandular or preferably retrofascial (between the fascia of the pectoral muscle and the pectoral muscle itself).
If we have a patient with a chest proportionate to height, with a well-shaped mammary gland and the nipple centered on the cup, who wants a homogeneous increase in volume, we can opt for both a round prosthesis and an anatomical prosthesis according to aesthetic preferences of the patient herself. Once the dimensions of the prosthesis have been chosen through measurements, the different projections will determine the final volume of the implant.
If, on the other hand, the patient is short and with a somewhat wide chest or vice versa she is rather tall and thin, even in the presence of a well-developed mammary gland, the most suitable prostheses will be the anatomical ones which, in addition to the teardrop shape, have the possibility of having a different height than the width, a feature that allows, after a careful evaluation by the surgeon, to be able to create a harmonious and natural breast based on the formation of the thoracic cage.
If the mammary gland presents a slight loss of tone (mammary ptosis) we use some technical measures aimed at lifting the breast such as the dual plane technique, associated, if it is necessary to also ascend the nipple, to an upper hemiperiareolar or complete periareolar surgical access with round block suture. We will also use anatomical prostheses with a high degree of projection and cohesion so that they themselves support the slightly ptotic mammary gland.
If the patient wants a quick return to sports and/or work activity and/or uses the upper limbs for work, we use polyurethane-coated prostheses that are fixed in a few days to the surrounding tissues in an immovable way, eliminating the risk of rotation, elevation or asymmetry of the prostheses themselves.
If the patient has already been operated on and wishes to replace the implants, we use polyurethane-coated prostheses because the risk of capsular contracture (the main complication linked to the insertion of breast implants) is very low and is around 2-4% 10 years after the intervention.
If the patient’s priority is to have the lowest possible medium / long-term risk of complications, we use polyurethane prostheses.
1. PHOTO BEFORE AND AFTER (anatomical retromuscular prosthesis)
We carry out the operation with a surgical access that can be from the inframammary sulcus or from the areola, positioning the prosthesis, as mentioned above, in the retroglandular, retrofascial, or retromuscular plane, using round or anatomical prostheses with varying degrees of projection and cohesion. All these variables depend both on the preoperative anatomical situation of the breasts and the wishes of the patient and are carefully evaluated during the preliminary interviews. If the mammary gland presents a modest loss of tone (the so-called mammary ptosis) we use some technical measures aimed at lifting the breasts such as the dual plane technique, associated, if it is necessary to ascend the nipple, to a surgical upper hemiperiareolar or complete periareolar access with tobacco bag suture (round block).
At the end of the surgery, we place two drains which are generally removed after 24 hours. The operation takes place under general anesthesia and lasts about an hour and a half / two hours and can be performed in a day hospital. Light sporting activity is recommended after a week to soften the periprosthetic capsule in formation.
MOST COMMON QUESTIONS AND ANSWERS FOR ADDITIVE MASTOPLASTY OPERATION
Is breast augmentation a painful surgery?
No, because anesthetic precautions are carried out before narcosis and painkilling therapy is prescribed at home. The patient may experience normal post-operative discomfort, which is easily controlled with analgesics; the discomfort may be slightly greater in the case of very large prostheses and/or if coated with polyurethane.
Will the silicone implant be visible?
Generally not, but it is clear that the larger the prosthesis, the greater the risk of its visibility and an unnatural result.
Are the drains necessary? Drains are not necessary, but scientific studies have shown that the removal of the minimum amount of serum blood that inevitably forms after each surgical procedure reduces the risk of capsular contracture, so we prefer to insert them and remove them after 12/24 hours.
What type of bra should I use after breast augmentation?
A sports bra is needed, if polyurethane prostheses are inserted, it can be removed after 20 days. Will the scar be visible? The periareolar scar is often practically invisible as after a few months some simple measures can be put in place so that it assumes the pigmentation of the areola itself, the one at the groove is visible if the groove is not covered by the gland itself, like a thin white line.
After the surgery, if the patient has a child, will she be able to breastfeed?
Yes, it is possible to breastfeed, but it is advisable only for a short time in order not to compromise the quality of the breast tissues and run the risk that the breasts “fall on the implants”, which obviously are fixed in the same position inside their capsule. If the patient intends to breastfeed, access to the inframammary sulcus is preferable in order not to compromise the gland.
Are the implants safe?
For over fifty years, mammoplasty has been constantly monitored by ultrasound, mammography, and nuclear magnetic resonance. We have known, for many years now, that implants not only do not increase the risk of breast cancer, but rather they are a protective factor because the prosthetic patient undergoes diagnostic tests more frequently, on average than the woman with natural breasts as she performs controls for both breast cancer screening and post-operative follow-up reasons.
Recently there have been discussions of an association between breast augmentation and anaplastic large cell lymphoma (ALCL). It is a rare form of lymphoma that affects both sexes, making up only 2% of all non-Hodkin’s lymphomas and which, if discovered in time and treated, has no consequences. Very rarely, this neoplasm can develop around a breast implant (BIA-ALCL, from Breast Implant-Associated Anaplastic Large Cell Lymphoma): the triggering causes are not known with certainty but, according to some hypotheses, there could be a correlation with a chronic inflammatory state due to the texturization of the implant, which would favor the degeneration of the T lymphocytes located in the vicinity of the prosthesis. On average, the diagnosis of this disease occurs 9-10 years after the prosthetic implant.
The alarm started a few years ago from France which reported some research data: in 2013, 130 cases on a worldwide basis, in 2014, 170 cases and from another source 177 cases in 2015. This is an extremely low incidence compared to the millions of women around the world who undergo breast augmentation every year. So, ultimately, in the current state of knowledge, we must take into account that, in the case of additive mammoplasty, there is a risk of anaplastic large cell lymphoma (BIA-ALCL). It is a rare tumor, perfectly treatable when caught in time. The symptoms are an abnormal swelling of the breast in the absence of obvious inflammatory events or trauma, supported by a late seroma (i.e. appeared at least 6 months after implantation): In this case, the patient must undergo sampling of at least 20cc of serum (with an ultrasound-guided probe) to be analyzed in a specialized center in order to exclude or confirm the diagnosis of lymphoma. In 2017, 12 deaths were reported from BIA-ALCL out of a total of 30 million women who have textured breast implants worldwide.
So, what real risk of death from BIA-ALCL does the patient who decides to introduce textured prostheses have?
To understand this even better, we can refer to the Micromort risk unit of measurement. The micromort measure was introduced in 1979 by Ronald A. Howard and a micromort indicates when a person’s risk of death is one in a million. For example, getting out of bed when you are 20 increases your risk of dying by one micromort, driving a car one hour a day increases your risk of dying by two micromorts, running a marathon increases your risk by 8 micromorts per run.
The risk of death from BIA-ALCL is 0.4 micromort for a woman with bilateral breast implants!
Do prostheses have a guarantee?
The most modern prostheses are guaranteed for life in case of breakage that is attributable to a structural defect and in this case, are replaced free of charge, some also offer promos for medical and hospitalization costs, others offer replacement even in the case of severe capsular contracture (Backer’s grade III and IV)
Hello, today I will talk to you about breast augmentation. Breast augmentation is a highly sought-after surgery and it is the surgery that, in my opinion, requires a great deal of dialogue between the surgeon and the patient because there are an infinite number of variables to be taken into account: the most important is the anatomical situation, the one that is the clinical situation of the patient, therefore her chest, her tissues, her gland; then there are the patient’s needs, those that are her desires but we have to see if her desires can be obtained on the basis of the patient’s anatomical and clinical situation.
Then there are the prostheses to choose from: they can be round or even anatomical; but also the surface of the prostheses today is very important and we need to talk about it carefully: there are smooth prostheses, medium smooth prostheses, rough prostheses and very rough prostheses (such as those in polyurethane); each has its advantages and disadvantages and also the choice of the type of prosthesis depends not only on the wishes of the patient but on the habits of the patient.
In addition, the prostheses can be placed in various planes: behind the muscle, only partially behind the muscle, behind the fascia, behind the gland, they can be inserted from the areola, a sulcus can be inserted, from the armpit. There’s an infinite number of variables, so there is a good dialogue, long, and constructive and eventually, if that is not enough, there is second a long and constructive meeting, in which tests are also carried out to verify if the appropriate dimension options are what the patient wants, because, in the end, she will bring them to herself.
If you have the need and pleasure to look at my site, it is www.lucacravero.it. You will see many photos and an explanation of what I have told you but most importantly, what you really need is the first visit. Until we meet again.
Breast augmentation (anatomical retroglandular prosthesis) before and after:




Breast augmentation (anatomic retromuscular prosthesis) before and after:




Breast augmentation (anatomic retromuscular prosthesis) before and after:






Breast augmentation (anatomic retromuscular prosthesis) before and after:








Breast augmentation (anatomic retromuscular prosthesis) before and after:





Breast augmentation (anatomic retromuscular prosthesis) before and after:





2. BEFORE AND AFTER PHOTOS (round prostheses)






Breast augmentation retrofascial anatomical prostheses 3 cup B before and after:






Breast augmentation retrofascial anatomic prosthesis 3 cup B before and after:






Round retromuscular breast augmentation before and after:






Breast augmentation (anatomic retromuscular prosthesis) before and after:




Before and after photographs with round dentures
Round retromuscular breast augmentation before and after:




Round retromuscular breast augmentation (Dual plane left breast)






Medium round retromuscular breast augmentation before and after:




Breast augmentation (round retromuscular prosthesis) before and after:






Breast augmentation (round retromuscular prosthesis) before and after:






Breast augmentation (round retromuscular prosthesis) before and after:




3. VIDEO CASES COMMENTARY
Breast Augmentation with Correction of Breast Hypoplasia
This is the case of a very young girl who has not only breast hypoplasia but also some degree of asymmetry. She wanted a non-bursting breast and by mutual agreement, we chose a round prosthesis passing through the areola, so as not to leave a visible scar at the height of the sulcus. We used prostheses of different volumes in order to try to restore the correct breast symmetry: in particular on the left a 285 cc prosthesis was used, on the right a 255 cc prosthesis. The plane is the retromuscular one.

Breast augmentation: a complex case
This is a rather complicated case of breast augmentation. The patient has a moderate degree of ptosis which can be remedied by placing an anatomical prosthesis at a certain degree of projection and preferably in the retro glandular plane since there is a good cutaneous texture, a good possibility of covering the prosthesis itself. In agreement with the patient, we decided to place a high-projection anatomical prosthesis in the retro-glandular site and at the same time, liposuction of the upper quadrants was performed, especially on the right breast, to be able to correct even a slight asymmetry. The one-year result is quite pleasant. The access is superior hemi-areolar: in this way, we were able to pull up the areola-nipple complex by an additional centimeter.
